
Structural spinal correction requires extensive post-doctoral training, and many Doctors undergo further diplomate training in addition. It is a unique focus within Chiropractic. The best analogy: we are the orthodontists of the spine. The most effective spinal corrective protocols may also be non surgical, when the outcome is health related quality of life, and ideal spinal alignment. Don’t misunderstand us. You don’t wait until you are looking at surgery to take care of your Spine. Quite the opposite. You need to take care of your spine long before the symptoms are so severe that you begin the several year process of finding and scheduling a surgical consult or surgery.
In fact, most health related quality of life issues have a lot to do with an improper spinal alignment as robustly indicated in medical literature. Many health conditions arise from postural / structural spine issues: migraines, headaches, poor immune function, allergies, back pains, asthma and allergies, poor or heavy cycles, erectile dysfunction, menstrual cramps, digestive issues, just to name a few!
Surgeries often leave patients in a same, or worsened, spinal alignment, due to lack of consideration of non surgical intervention. Our approach to structural correction implores medical consensus, literature, and various spine care techniques. We utilize biophysics principles combined with the latest physiology, mirror positioning, neuromuscular and neurological facilitation and input. The best of equipment and protocols from pettibon, chiropractic biophysics, clear scoliosis, diversified, gonstead, thompson, and other techniques are utilized as necessary.
The following explanations, adopted mostly by idealspine.com (Chiropractic BioPhysics website) gives a clear and concise vantage point of our approach and medical protocols. A “frame of reference” is provided for you to begin to understand and conceptualize why and how we are imploring our advanced analysis, treatment, rehabilitation and proactive active wellness care that follows.
Various pieces of unique equipment seen in true spinal correction clinics, of which there are few. We employ certified CBP practitioner(s) with advanced training in the state of Pennsylvania & New York.







CBP® Technique emphasizes optimal posture and spinal alignment as the primary goals of chiropractic care while simultaneously documenting improvements in pain and functional based outcomes (See Figure 1). The uniqueness of CBP® treatment is in structural rehabilitation of the spine and posture. In general the goals of CBP® Care are:
- Normal Front & Side View Posture
- Center of mass of head, rib cage & pelvis vertically aligned in Front and Side views.
- Normal Spinal Alignment
- Front view: vertical alignment
- Side View: Harrison Ideal or Average Spinal Model
- Normal function
- Improved Range of Motion and quality of movement,
- Improved muscle strength,
- Improved Health & Symptom Improvements
- Neck disability index
- Oswestry low back index,
- SF 36 or Health Status Questionnaire
IDEAL POSTURAL ALIGNMENT

Figure 1. Ideal postural alignment is depicted in both the frontal and side views. In each view, the center of mass of the skull, thorax, and pelvis are in a vertical line with respect to gravity. In the frontal view, the spinal column is vertically aligned-a straight column- with respect to gravity. In the side view, the spine has three primary curvatures which will be described below:
1. Neck Curve – Cervical Lordosis,
2. Ribcage Curve – Thoracic Kyphosis,
3. Low back Curve – Lumbar Lordosis
IDEAL SPINAL ALIGNMENT: HARRISON FULL SPINE MODEL
As in all fields of study dealing with the human body, i.e. physiology, hematology, anatomy, etc., there exist normal values for alignment of the spine. The Harrison Spinal Model is an evidenced based model for side view spinal alignment. It is the geometric path of the posterior longitudinal ligament or the backs of the vertebra from the 1st neck vertebra to the bottom of the lower back or top of the sacrum. See Figures 2-6 below detailing the Harrison Spinal Model.
CBP® researchers have extensively published ideal and average models for the human spinal curvatures as viewed from the side. This research has lead to the finding of the ‘Harrison Spinal Model’. This model details both Ideal and Average geometric shapes for the curves of the spine from the side. Additionally, ideal and average ranges for the spinal segmental angles for each of the spinal regions have been identified. The neck or cervical spine should have a geometric shape that approximates a ‘piece of a circle’. The ribcage or thoracic spine should have a geometric shape that approximates an oval-elliptical shape. And the low back or lumbar spine should have a geometric shape that approximates an oval-elliptical shape.26-31
These are “evidence based” models. In fact, the CBP® neck-cervical circular model27 and the low back- lumbar elliptical model29 have both been found to have discriminative validity between pain and non pain subjects. In other words, the Harrison Spinal Model has been found to be able identify pain subjects versus non-pain subjects by what their spinal x-ray shapes are.

Figure 3. These three figures demonstrate the concept that each spinal region has a normal geometry or shape of the spinal curves. On the readers left is the Neck or Cervical spine-Here the shape in the neck curve should approximate a piece of a circle. In the Center is the Ribcage or Thoracic spineHere the shape in the ribcage should approximate a piece of an oval or ellipse. On the Right is the Low back or Lumbar spine. Here the shape in the low back should approximate a piece of an oval or ellipse.
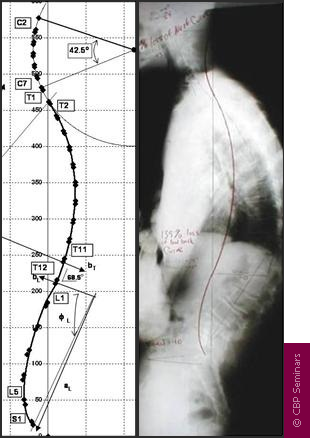
Figure 4. The Harrison Full Spine Model. On the readers left is the exact geometric model of the side view of the spinal curves as identified by Harrison and colleagues. This model can be used to determine what is wrong-abnormal with a given patients side view of the spine. For example, a full spine x-ray on the right is shown. The red-curved line represents the Harrison spinal model and this shows where the patients spinal vertebra should be lined up. It is apparent that this patient has altered spinal alignment as they do not fit even close to the Harrison Idealized Spinal Model.

Figure 5. The Harrison Spinal Model in the Neck-Cervical region. The Harrison spinal model is depicted as the GREEN curved line in this figure. On the Right is a normal curved patient x-ray. On the Left is an abnormal curved patient x-ray; where the patients abnormal shape is shown by the Red dashed line. The Harrison Spinal Model in the neck has been shown to reasonably predict which person will have neck pain compared to normal subjects.
Figure 6. The Harrison Spinal Model in the Low back or Lumbar region. The Harrison spinal model is depicted as the RED curved line in this figure. On the Right is a normal curved patient x-ray. On the Left is an abnormal curved patient x-ray; where the patients abnormal shape is shown by the faint dashed line. The Harrison Spinal Model in the low back has been shown to reasonably predict which person will have low back pain compared to normal subjects.
X-RAY ANALYSIS AND UTILIZATION
To establish optimal and average sagittal models, x-ray analysis and line drawing procedures are utilized. CBP® protocols require that the doctor must measure the displacements on spinal radiographs (segmental Subluxation). Both lateral-side view and anterior to posterior (AP) or frontal view CBP® x-ray line drawing procedures have been studied and found to be reliable.32-36 Furthermore, CBP® utilizes standardized x-ray positioning procedures that have been studied and found to be reliable.36
As with measures of pain intensity, range of motion, and quality of life, periodic assessment of spinal structural alignment is important to evaluate progress and determine when maximum patient improvement has been reached. In CBP® Technique, the use of initial and follow-up spinal x-rays or radiographs is deemed necessary; however, some in chiropractic have condemned the use of follow-radiographs to collect alignment data.37-39 Importantly, there is data to show that the use of medical/chiropractic x-rays constitutes a very minor health risk and in fact has been shown to be of benefit (decreased sickness and cancer mortality rates) in some studies.40-42
In reality, the only way to see what an individual patients spine alignment looks likes, is to obtain spinal imaging such as Radiography or X-ray. No-one would not take their car to the mechanic and say: Something’s wrong with my engine but don’t look under the hood–Would you? Then why would anyone want a Chiropractor to adjust-treat their spine without having an x-ray to see what the person’s spine looked like? Would You?
CBP® POSTURAL ANALYSIS
Previously, engineering concepts were used to describe all spinal-vertebral segmental movements as rotations and translations in 3-dimensions.10 However, Dr. Don Harrison was the first to describe abnormal postures of the head, rib cage, and pelvis in this manner.1-3,9 Figures 7 and 8 depict the twelve simple motions in six-degrees of freedom as rotations and translations of the human head, ribcage, and pelvis:
- Rotation is a turning, twisting, or tilting movement and is an angular movement
- Translation is a straight line movement (up, down, left, right, forward, backward)
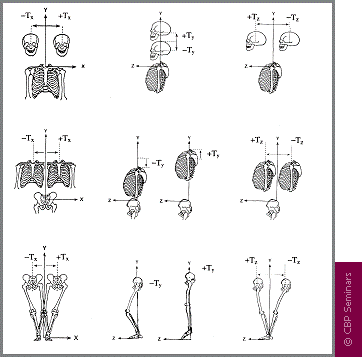
Figure 7. The possible translation postures (Tx, Ty, Tz) of the head, rib cage, and pelvis are depicted in 3-dimensions. In 1980, Dr. Don Harrison termed these pairs on any one axis as Mirror Images®. Whichever Abnormal postures were found to exist in the patient, these postures would be placed into their Mirror Image® before a force was applied with an adjusting instrument, drop table, exercise and/or traction.
Figure 8. The possible postural rotations (Rx, Ry, Rz) of the head rib cage and pelvis are depicted in 3-dimensions. In 1980, Dr. Don Harrison termed these pairs on any one axis as Mirror Images®. Whichever postures were found to exist in the patient, these postures would be placed into their Mirror Image® before a force was applied with an adjusting instrument, drop table, exercise and/or traction.
The postural and spinal displacements are the determining factors for deriving a patients individualized program of care. Prior to performing CBP® Mirror Image® postural set-ups, the patients initial presenting abnormal posture(s) must be exactly determined. Ideal posture can be precisely described as vertical alignment of the centers of mass of the head, ribcage, and pelvis with respect to gravity (Figure 1 above). In other words, none of the rotations and translations in Figures 7 and 8 can be present. Using this definition, abnormal postural rotations and translations can be determined.
MIRROR IMAGE® POSTURAL ADJUSTMENTS
In March 1980, Dr. Don Harrison originated postural Chiropractic adjusting procedures that he coined Mirror Image®. Clinically, these adjusting set-ups were found to result in postural and spinal alignment improvements verified with follow up x-ray; this impression would be subjected to studies later as shown in Table 1 above.
For each of these postures illustrated in Figures 7 and 8, Dr. Don Harrison and his brother Glenn Harrison originated drop table adjustments, instrument adjustments (both table and hand-held). For these new Mirror Image® patient positions, Dr. Don Harrison placed the patient in their opposite posture. These Harrison Mirror Image® positions can be described as reflecting the patients head, rib cage, and/or pelvis across the median-sagittal plane in the AP view, and positioning the head, rib cage, and/or pelvis across the mid-frontal plane in the lateral view.9 Figures 9 and 10 demonstrate two examples (there are literally thousands more as there can be many postural combinations of each region) of Mirror Image® Adjustments utilized in CBP® Technique.
Mirror Image Adjustments, assists the Chiropractor in the rehabilitation of the patients posture. In theory, these adjustments re-balance the bodies sense of proper balance or alignment by way of triggering improved muscle and nerve reflexes. Thus, postural adjustments as performed with drop table, hand-held instrument, or even mirror image manipulation procedures, are performed for resetting the nervous system regulation of postural muscle balance.51

Figure 9. Mirror Image adjustment example for the head posture. The patient has forward head posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is the CBP Mirror Image adjustment. The posture is placed in its opposite position and then a Chiropractic adjustment is performed.

Figure 10. Mirror Image adjustment example for the ribcage posture. The patient has right lateral ribcage posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is the CBP® Mirror Image adjustment. The posture is placed in its opposite position and then a Chiropractic adjustment is performed.
MIRROR IMAGE® POSTURAL EXERCISES
Further, in 1980-1986, Dr. Don and Dr. Glenn Harrison began developing and testing Mirror Image®posture exercises.1-3 Mirror image® exercises are performed to stretch shortened muscles and to strengthen those muscles that have weakened in areas where postural muscles have adapted to asymmetric abnormal postures. Although strength and conditioning exercise has not proven to correct posture,46 postural exercises performed in the mirror image have shown initial promise in the reduction of posture and spinal displacements.47-50 Figures 11 and 12 demonstrate Corrective Mirror Image exercises for the same postures as in Figures 10-11.

Figure 11. Mirror Image exercise example for the abnormal forward head posture. The patient has an abnormal forward head (translation) posture and the skeletal animation shows what happens to the spine with this posture. On the right is two different CBP® Mirror Image exercisesone with just the patients muscles and body as resistance and the other with an elastic band for increased contraction effort. The patient actively maneuvers their posture into the opposite or Mirror Image position.

Figure 12. Mirror Image exercise example for an abnormal lateral shifted (translated) ribcage posture. The patient has right lateral ribcage posture (translation) and the skeletal animation shows what happens to the spine with this posture. On the right is two different CBP® Mirror Image exercises one with just the patient s muscles and body as resistance and the other with an elastic band for increased contraction effort. The patient actively maneuvers their posture into the opposite or Mirror Image position.
MIRROR IMAGE® POSTURAL AND SPINAL TRACTION
Additionally from 1980-1986, for use in difficult cases, Dr. Don Harrison and Dr. Glenn Harrison originated several Mirror Image® postural traction (rotations and translations of the head, rib cage, and pelvis) and cervical extension (backwards bending) traction methods to restore the sagittal cervical curve. These CBP® Technique cervical extension traction methods were improved upon over the years by several other CBP® practitioners.
From 1996-2000, several postural and spinal traction methods to restore thoracic and lumbar sagittal curvatures were developed by Dr. Deed Harrison; Dr. Don Harrisons son.11-13 Dr. Deed began to further refine the CBP® Technique cervical traction methods with an analysis of head posture, curve configuration, thoracic curvature, gender, and body size.4 From 1992-2004, six non-randomized clinical control trials,13-18 one randomized clinical control trial,19 and five case studies20-24 have been performed on these CBP® Technique Mirror Image® procedures.
Postural mirror image and extension traction for the side view spinal curves provides sustained loading periods of 10-20 minutes and is necessary to cause visco-elastic deformation to the resting length of the spinal ligaments, muscles, and discs.52 In clinical controlled trials, extension traction, as done in CBP® Technique, is the only proven method (without surgery) shown to consistently correct abnormal spinal curvatures back towards their normal alignment.
There are MANY types of spinal extension traction methods used in CBP® Technique; some are more aggressive and technical than others. Whereas some forms of spinal extension traction are available for patients to use at home; the examples shown in Figures 13-14 are in office types only. Note: Each patients spine is unique and thus, a variety of traction devices are used depending upon the exact condition of the patient.
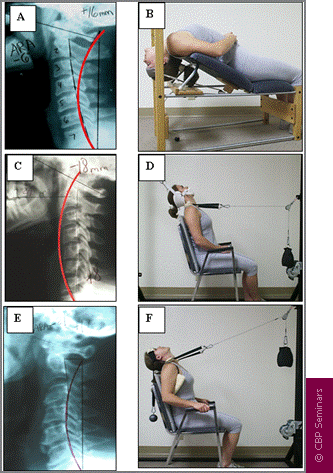
Figure 13. Three different subluxations (abnormal alignment) of the cervical curve and their respective Mirror Image traction methods. In A, hypolordosis with mild anterior head translation requires compression extension traction in B. In C, slight kyphosis with posterior head translation requires 2-way non-compression traction in D. In E, reversal of the upper cervical curve with mild anterior head translation requires compression extension 2-way traction in F.4,14-16
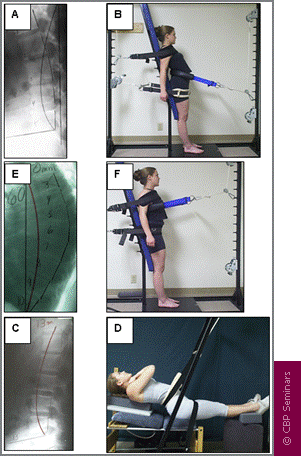
Figure 14. Two different subluxations of the lumbar curve and one of the thoracic curve and their respective Mirror Image traction methods. In A, lumbar kyphosis with anterior thoracic translation requires 3-point bending extension traction in B (shown standing). In C, slight lumbar kyphosis with posterior thoracic translation requires 3-point bending in D (shown supine). In E, hyper-kyphosis of the thoracic curve requires 3-point bending thoracic traction in F (shown standing).
TREATMENT INTERVENTIONS
The CBP® protocol of care recommends that relief care (traditional chiropractic management) be separated from structural rehabilitation of the spine and posture. In this regard, the typical patient would receive an initial 3 weeks of care (4 times per week or 12 visits) aimed at improving segmental and overall spinal range of motion (RoM) and pain intensity/frequency. Treatment interventions/methods would consist of any number of segmental adjusting techniques the chiropractor prefers to utilize (Diversified, Gonstead, Activator, etc ).
After, the initial relief care examination (average 12 visits), CBP® structural rehabilitation procedures would begin and include Mirror Image® exercises, adjustments, and traction (referred to as the E.A.T protocol). The mirror image® posture positions are the rotation and translation pairs in or about each coordinate axis (Figures 3 and 4 above). Thus, CBP® care is multi-modal and is consistent with Bolton’s ideas of clinical applications in evidence based practice.45 Table 2 outlines treatment interventions recommended by CBP® for each of relief and structural rehabilitative care.
The reason for postural mirror image exercises, adjustments, and traction procedures is to address all the tissues involved in spine and posture alignment.
Unlike the relief care phase (approximately 12 visits), which includes segmental adjusting procedures from other named techniques, the E.A.T corrective care protocol is unique to CBP®. In combination, these E.A.T. methods are unique to CBP® Technique.
TABLE 2
CBP® recommended treatment methods for each phase of care, relief and structural rehabilitation of the spine and posture.
Relief Care or Standard Chiropractic Care |
CBP® Technique Structural Rehabilitation
|
||
| Intervention | Determination | Intervention | Determination |
| Spinal Manipulative Therapy | Palpatory Pain and Range of Motion | Mirror Image® Adjustment | PosturePrint® & Clinical Visualization |
| Spinal Stretching | Range of Motion | Mirror Image® Exercise | PosturePrint® & Clinical Visualization |
| Ice / Heat | Injury / Inflammation | Mirror Image® Postural Traction | PosturePrint® & Clinical Visualization |
| Mirror Image® Sagittal Curve Traction | Lateral View X-Ray (PostureRay® X-Ray Digitalization Preferred) | ||
FREQUENCY & DURATION OF CBP® TECHNIQUE CARE
Previously it was stated that a typical patient is started with relief care at a frequency of 4 times per week for 3 weeks or 12 visits. After this 12 visit relief care regiment, a patient is re-evaluated to document improvements in initial (visit 1) positive exam findings, pain scales, disability indices, health status, and range of motion. Following this re-evaluation, the patient is transitioned into CBP® structural rehabilitative E.A.T. procedures.4
To determine if the CBP® E.A.T protocol of corrective care for each individual (based on his/her posture and spinal displacements) is achieving the desired normalization of posture and spinal alignment, re-examinations are suggested at 36 visit intervals. In other words after 24 visits of CBP® E.A.T interventions added to the initial 12 visits of relief care. This 36 visit number is not based on personal opinion, but rather is an average duration from our six CBP® clinical control trials.13-18 In order to arrive at this 36 visit time period, one could use a frequency of 4 visits per week for 9 weeks or 3 visits per week for 12 weeks.
In six clinical control trials detailing the outcomes of chronic pain patients with CBP® Treatment interventions, the average chronic pain patient achieved a 75-80% improvement in their chronic pain and a 50% correction of their initial subluxated (abnormal spine alignment) position towards ideal and average spine alignment.13-18 This data indicates that, on average, a typical chronic pain patient may need 2 blocks of 36 visits of intensive structural rehabilitative care (defined as 3 or 4 visits per week) to achieve as near normal spinal alignment as possible.
TABLE 3
CBP® Protocol and Phases of Care showing the timing of different Treatment methods.
The frequency and duration of further care recommended to the patient at the 36 visit re-evaluation depends on their improvement in both structural and functional based outcomes. For example, if a patient achieves near-normal posture and spinal alignment at the 36 visit re-evaluation, then a reduced frequency of treatment is recommended for stabilization care (1-4 times per month depending upon the case). However, if at the first corrective care re-evaluation, less than average improvement is attained on comparative radiographs and postural examination (PosturePrint), then this is indication that another block of 36 visits may be necessary for continued spinal correction. With CBP®’s six completed clinical control trials, our methods have moved from the clinical opinion arena to having foundation in the category of evidence based care.
CONCLUSION
In our present era, evidence-based medicine was coined as a means to improve patient outcomes and quality of care. CBP® Technique uses postural and radiographic analysis procedures that have been shown to be reliable and valid. Significantly, CBP® Technique has multiple types of peer-reviewed publications in scientific journals as evidence for its patient treatment methods. What remains for CBP® technique is further refinement of technique protocols and evaluating the effects of subluxation reduction using the E.A.T. procedures in more advanced study designs. CBP is a technique practiced by a large number of practitioners, is a leader in the chiropractic technique and biomechanics research arena, and has shown good potential to improve chronic pain conditions in several patient populations and selected case studies.
Links & Resources
Origin: https://idealspine.com/cbp-research/
A primary source of information for the major framework of our protocols comes from ideal spinal models. A lot of work in this arena has been done by various authors. In the correction based arena, we follow many of the protocols and advancements done by the top authorities on Spinal alignment. One of those we refer to often is Chiropractic Biophysics Non-profit, Inc. is a 501(c)(3) nonprofit corporation dedicated to the advancement of chiropractic principles through scientific research. Dr. Don Harrison (deceased) and his second wife Dr. Deanne LJ Harrison (deceased) founded CBP research foundation in 1982; it was registered as CBP Non-Profit, Inc. in 1989 by Dr. Sang Harrison (Don’s 3rd and final life’s love). Through this organization Dr. Don and colleagues have published 140 peer-reviewed spine and Chiropractic research publications. Further, CBP Non-Profit, Inc. has funded many scholarships as well as donated chiropractic equipment to many chiropractic colleges; always trying to support chiropractic advancement and education. Dr. Don Harrison was the acting president of CBP Non-Profit, Inc. since 1982. Currently, Dr. Deed Harrison (Don’s son) is the President of CBP Non-Profit, Inc.
Results of our studies have been published in prestigious research journals and presented at respected conferences around the world. Your (Chiropractic donations) support enables us to continue important research and gives you a voice in the course our studies take. Join today, either as a regular member or member of the President’s Circle. The result will be better chiropractic techniques, stronger chiropractic practices, and healthier chiropractic patients.
CBP® RESEARCH CONSISTS OF STUDIES ON A VARIETY OF CBP® TECHNIQUE RELATED TOPICS INCLUDING:
- Spine modeling studies evaluating ideal and average human alignment variables,
- Spine biomechanics studies analyzing loads, stress, and strains,
- Posture modeling studies,
- Reliability of measurements and evaluation of patients (x-ray, posture),
- Validity of the measurements and evaluation of patients,
- Randomized trials evaluating technique outcomes
- Non-randomized trials evaluating technique outcomes,
- Case series studies evaluating technique outcomes,
- Case studies evaluating technique outcomes,
- Literature reviews and professional commentaries.
CBP® PEER-REVIEWED CLINICAL INVESTIGATIONS LISTED BY STUDY DESIGN / TYPE
Randomized Clinical Trials (RCT’s)
1. Zaleski BW, Wood J. A comparison of Palmer package and Chiropractic Biophysics for the treatment of pain. Proceedings of the International Conference on Spinal Manipulation 1992; Chicago, IL., May 15-17. 2. Moustafa IM, Diab AA. Rehabilitation for Pain and Lumbar Segmental Motion in Chronic Mechanical Low Back Pain: A Randomized Trial. Journal of Manipulative and Physiological Therapeutics Volume 35, Issue 4 , Pages 246-253, May 2012. 3. Moustafa IM, Diab AA. Extension traction treatment for patients with discogenic lumbosacral radiculopathy: a randomized controlled trial. Clin Rehabil June 8, 2012 Published online before print June 8, 2012.
Non-Randomized Clinical Trials (N-RCT’s)
4. Grimston SK, Engsberg JR, Shaw L, Vetanze NW. Muscular rehabilitation prescribed in coordination with prior chiropractic therapy as a treatment for sacroiliac subluxation in female distance runners. Chiropractic Sports Med 1990; 4(1):2-8. 5. Harrison DE, Harrison DD, Cailliet R, Janik TJ, Holland B. Changes in Sagittal Lumbar Configuration with a New Method of Extension Traction: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002;83(11):1585-1591. 6. Harrison DD, Jackson BL, Troyanovich SJ, Robertson GA, DeGeorge D, Barker WF. The Efficacy of Cervical Extension-Compression Traction Combined with Diversified Manipulation and Drop Table Adjustments in the Rehabilitation of Cervical Lordosis. J Manipulative Physiol Ther 1994;17(7):454-464. 7. Harrison DE, Harrison DD, Betz J, Colloca CJ, Janik TJ, Holland B. Increasing the Cervical Lordosis with Seated Combined Extension-Compression and Transverse Load Cervical Traction with Cervical Manipulation: Non-randomized Clinical Control Trial. J Manipulative Physiol Ther 2003; 26(3): 139-151. 8. Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. New 3-Point Bending Traction Method of Restoring Cervical Lordosis Combined with Cervical Manipulation: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002; 83(4): 447-453. 9. Harrison DE, Harrison DD, Haas JW, Betz JW, Janik TJ, Holland B. Conservative Methods to Correct Lateral Translations of the Head: A Non-randomized Clinical Control Trial. J Rehab Res Devel 2004;41(4):631-640. 10. Harrison DE, Cailliet R, Betz JW, Harrison DD, Haas JW, Janik TJ, Holland B. Harrison Mirror Image Methods for Correcting Trunk List: A Non-randomized Clinical Control Trial. Eur Spine J 2004; Euro Spine J 2005; 14(2):155-162.
CBP Published Case Studies
Chiropractic Pediatrics by Year
11. Peet J. Brachial plexus injury in an infant with Down’s syndrome: A case study. Chiropractic Pediatrics 1994; 1(2):11-14. 12. Marko SK. Case study: The effect of chiropractic care in an infant with problems of Constipation. Chiropractic Pediatrics 1994 ; 1:23-24. 13. Garde R. Asthma & Chiropractic. Chiropractic Pediatrics 1994; 1(3): 9-16. 14. Marko R. Bedwetting: Tow Case Studies. Chiropractic Pediatrics 1994; 1(2): 21-22. 15. Krauss L. Case Study: Infants inability to breast feed. Chiropractic Pediatrics 1994; 1(3):27. 16. Peet J, Marko SK, Piekarczk W. Chiropractic response in the pediatric patient with Asthma: A Pilot Study. Chiropractic Pediatrics 1995; 1(4):9-13. 17. Krauss L. Case Study: Birth Trauma resulting in colic. Chiropractic Pediatrics 1995; 2(1):10-11. 18. Marko R. Chiropractic Biophysics Technique in care of a child with Otitis Media. Chiropractic Pediatrics 1996; 2(2):13&26. 19. Marko SK. Adjusting the newborn infant with Jaundice. Chiropractic Pediatrics 1996; 2(3):9-10. 20. Peet J. Case Study: Chiropractic results with a child with reoccurring Otitis Media accompanied by Effusion. Chiropractic Pediatrics 1996; 2(2):8,11, & 12. 21. Peet J. Adjusting the Febrile pediatric patient. Chiropractic Pediatrics 1996; 2(3):11-12. 22. Peet J. Adjusting the Hyperactive/A.D.D. pediatric patient. Chiropractic Pediatrics 1997; 2(4):12-13, 16. 23. Peet J. Case study: Three year old female with acute stomach problems. Chiropractic Pediatrics 1997; 3(1):10-11. 24. Peet P. Child with chronic illness: Respiratory Infections, ADHD, and fatigue response to chiropractic care. Chiropractic Pediatrics 1997; 3(1):12-13. 25. Marko SK. Case Study: Ten year old male with severe Asthma. Chiropractic Pediatrics 1997; 3(2):6-8. 26. Peet J. Case Study: Eight year old female with chronic Asthma. Chiropractic Pediatrics 1997; 3(2):9-12. 27. Marko RB. A case study: Four year old female with Vesicoureteral Reflux. Chiropractic Pediatrics 1998; 3(3):12-13. 28. Marko SK. Case Study: Sven year old female with Asthma, Constipation, and Headaches among other symptoms. Chiropractic Pediatrics 1998 4(1):14-15.
Index Medicus & ICL Case Studies
29. Harrison DE, Bula JB. Non-operative correction of flat back using lumbar extension traction: A case study of three. J Chiropractic Education 2002;16(1). 30. Troyanovich SJ, Buettner M. A structural chiropractic approach to the management of diffuse idiopathic skeletal hyperostosis. J Manipulative Physiol Ther 2003;26:202-206. 31. Colloca CJ, Polkinghorn BS. Chiropractic management of Ehlers-Danlos Syndrome: A report of two cases. J Manipulative Physiol Ther 2003;26:448-459. 32. Paulk GP, Bennett DL, Harrison DE. Management of a chronic lumbar disk herniation with CBP methods following failed chiropractic manipulative intervention. J Manipulative Physiol Ther 2004; 27(9): 579e1-579e7. 33. Bastecki A, Harrison DE, Haas JW. ADHD: A CBP case study. J Manipulative Physiol Ther 2004; 27(8): 525e1-525e5. 34. Ferrantelli JR, Harrison DE, Harrison DD, Steward D. Conservative management of previously unresponsive whiplash associated Physiol Ther 2005; 28(3):e1-8. 35. Haas JW, Harrison DE, Harrison DD, Bymers B. Reduction of symptoms in a patient with syringomyelia, cluster headaches, and cervical kyphosis. J Manipulative Physiol Ther 2005; 28(6):452. 36. Oakley PA, Harrison DE. Use of Clinical Biomechanics of Posture (CBP) protocol in a postsurgical C4-C7 total fusion patient. A case study. J Chiropractic Education 2005;19(1):66. 37. Harrison DE, Oakley PA, Harrison DD. Reduction of deformity after chiropractic biophysics mirror image care incorporating the non-commutative property of finite rotation angles in five patients with thoracolumbar scoliosis. J Chiropractic Education 2006;20(1):19-20. 38. Fedorchuk C. Correction of subluxation and reduction of dyspnea in a 7 year-old child suffering from chronic cough and asthma: A case report. J Vertebral Subluxation Res 2007; November 28: 1-5. 39. Berry RH, Oakley PA, Harrison DE. A structural approach to the postsurgical laminectomy case. J Vert Sublux Res 2007; March 19:1-7. 40. Fedorchuk C. Case Report: Treatment and Recovery of a Patient Suffering From Muscular Dystrophy, and Hypertension Utilizing Chiropractic Care. JVSR 2008; No.26:5-6. 41. Fedorchuk C, Cohen A. Resolution of Chronic Otitis Media. J Ped Mat Family Health Chiropractic 2009; No.2: 1-8. 42. Fedorchuk C, Wheeler G. Resolution of Headaches in a 13 Year-Old Following Restoration of Cervical Curvature Utilizing Chiropractic Biophysics: A Case Report. J Ped Mat Family Health Chiropractic 2009; Nov. 30: 1-7. 43. Cardwell A, Ferrucci M, Harrison DE. Chiropractic BioPhysics® (CBP®) Protocol on a Patient with Tourette’s syndrome, Tardive Dyskinesia, CREST syndrome, and Fatigue. JVSR 2009;. 44. Fedorchuk C, Wetterlin JK, McCoy M. Reduction of subluxation using CBP technique and improvement of childhood idiopathic scoliosis: A series of seven cases. J. Pediatric Maternal & Family Health 2010; Dec. 9:220-222. 45. Fedorchuk C, Burk L, Phillips SL. Reduction in Cholesterol and Improved Quality of Life in a Patient with Dyslipidemia Undergoing Chiropractic Care: A Case Study. Annals Vertebral Subluxation Res. 2011; June 2: 26-36. 46. Fedorchuk C, St. Bernard A. Improvement in Gastro Esophageal Reflux Disease Following Chiropractic Care and the ALCAT Procedure. Annals of Vertebral Subluxation Research ~ June 23, 2011 ~ Pages44-50
X-Ray Reliability Studies
47. Jackson BL, Harrison DD, Robertson GA, Barker WF. Chiropractic Biophysics Lateral Cervical Film Analysis Reliability. J Manipulative Physiol Ther 1993;16(6): 384-91. 48. Troyanovich SJ, Robertson GA, Harrison DD, Holland B. Intra- and Interexaminer Reliability of the Chiropractic Biophysics Lateral Lumbar Radiographic Mensuration Procedure. J Manipulative Physiol Ther 1995;18(8):519-524. 49. Troyanovich SJ, Harrison DE, Harrison DD, Holland B, Janik TJ. A Further Analysis of the Reliability of the Posterior Tangent Lateral Lumbar Radiographic Mensuration Procedure: Concurrent Validity of Computer Aided X-ray Digitization. J Manipulative Physiol Ther 1998; 21(7): 460-467. 50. Troyanovich SJ, Harrison SO, Harrison DD, Harrison DE, Payne M, Janik TJ, Holland B. Chiropractic Biophysics Digitized Radiographic Mensuration Analysis of the Anteroposterior Lumbar View: A Reliability Study. J Manipulative Physiol Ther 1999; 22(5): 309-315. 51. Troyanovich SJ, Harrison DE, Harrison DD, Harrison SO, Janik TJ, Holland B. Chiropractic Biophysics Digitized Radiographic Mensuration Analysis of the Anteroposterior Cervico- thoracic View: A Reliability Study. J Manipulative Physiol Ther 2000; 23: 476-82. 52. Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ, Holland B. Cobb Method or Harrison Posterior Tangent Method: Which is Better for Lateral Cervical Analysis? Spine 2000; 25(16): 2072-78. 53. Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Centroid, Cobb or Harrison Posterior Tangents: Which to Choose for Analysis of Thoracic Kyphosis? Spine 2001; 26(11): E227-E234. 54. Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Radiographic Analysis of Lumbar Lordosis: Cobb Method, Centroidal Method, TRALL or Harrison Posterior Tangents? Spine 2001; 26(11): E235-E242. 55. Janik TJ, Harrison DE, Harrison, DD, Payne MR, Coleman RR, Holland B. Reliability of lateral bending and axial rotation with validity of a New Method to determine Axial Rotations on AP Radiographs. J Manipulative Physiol Ther 2001; 24(7): 445-448. 56. Harrison DE, Holland B, Harrison DD, Janik TJ. Further Reliability Analysis of the Harrison Radiographic Line Drawing Methods: Crossed ICCs for Lateral Posterior Tangents and AP Modified Risser-Ferguson. J Manipulative Physiol Ther 2002; 25: 93-98. 57. Normand MC, Harrison DE, Cailliet R, Black P, Harrison DD, Holland B. Reliability and Measurement Error of the BioTonix Video Posture Evaluation System. Part I: Inanimate objects. J Manipulative Physiol Ther 2002; 25(4): 246-250. 58. Harrison DE, Harrison DD, Colloca CJ, Betz JW, Janik TJ, Holland B. Repeatability Over Time of Posture, X-ray Positioning, and X-ray Line Drawing: An Analysis of Six Control Groups. J Manipulative Physiol Ther 2003; 26(2):87-98. 59. Harrison DE, Haas JW, Cailliet R, Harrison DD, Janik TJ, Holland B. Concurrent Validity of the Flexicurve Instrument Measurements: Sagittal Skin Contour of the Cervical Spine Compared to Lateral Cervical radiographic Measurements. J Manipulative Physiol Ther 2005; 28(8):597-603. 60. Harrison DE, Haas JW, Harrison DD, Janik TJ, Holland B. Sagittal Skin Contour of the Cervical Spine: Inter-examiner and Intra-examiner Reliability of the Flexicurve Instrument. J Manipulative Physiol Ther 2005; 28(7):516-9.
Spinal Modeling / Biomechanics Studies
61. Harrison DD, Janik TJ, Troyanovich SJ, Holland B. Comparisons of Lordotic Cervical Spine Curvatures to a Theoretical Ideal Model of the Static Sagittal Cervical Spine. Spine 1996;21(6):667-675. 62. Harrison DD, Janik TJ, Troyanovich SJ, Harrison DE, Colloca CJ. Evaluations of the Assumptions Used to Derive an Ideal Normal Cervical Spine Model. J Manipulative Physiol Ther 1997; 20(4): 246-256. 63. Troyanovich SJ, Cailliet R, Janik TJ, Harrison DD, Harrison DE. Radiographic Mensuration Characteristics of the Sagittal Lumbar Spine From A Normal Population with a Method to Synthesize Prior Studies of Lordosis. J Spinal Disord 1997;10(5): 380-386. 64. Harrison DD, Cailliet R, Janik TJ, Troyanovich SJ, Harrison DE, Holland B. Elliptical Modeling of the Sagittal Lumbar Lordosis and Segmental Rotation Angles as a Method to Discriminate Between Normal and Low Back Pain Subjects. J Spinal Disord 1998; 11(5): 430-439. 65. Janik TJ, Harrison DD, Cailliet R, Troyanovich SJ, Harrison DE. Can the Sagittal Lumbar Curvature be Closely Approximated by an Ellipse? J Orthop Res 1998; 16(6): 766-770. 66. Harrison DE, Harrison DD, Janik TJ, Jones EW, Cailliet R, Normand M. Comparison of Axial and Flexural Stresses in Lordosis and Three Buckled Modes in the Cervical Spine. Clin Biomech 2001; 16(4): 276-284. 67. Harrison DD, Jones EW, Janik TJ, Harrison DE. Evaluation of Flexural Stresses in the Vertebral body Cortex and Trabecular Bone in Three Cervical Configurations with an Elliptical Shell Model. J Manipulative Physiol Ther 2002; 25(6): 391-401. 68. Harrison DE, Janik TJ, Harrison DD, Cailliet R, Harmon S. Can the Thoracic Kyphosis be Modeled with a Simple Geometric Shape? The Results of Circular and Elliptical Modeling in 80 Asymptomatic Subjects. J Spinal Disord 2002; 15(3): 213-220. 69. Harrison DE, Harrison DD, Janik TJ, Cailliet R, Haas JW. Do alterations in vertebral and disc dimensions affect an elliptical model of the thoracic kyphosis? Spine 2003; 28(5):463-469. 70. Keller TS, Harrison DE, Colloca CJ, Harrison DD, Janik TJ. Prediction of osteoporotic spinal deformity. Spine 2003; 28(5): 455-462. 71. Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW, Ferrantelli J, Holland B.Modeling of the Sagittal Cervical Spine as a Method to Discriminate Hypo-Lordosis: Results of Elliptical and Circular Modeling in 72 Asymptomatic Subjects, 52 AcuteNeck Pain Subjects, and 70 Chronic Neck Pain Subjects. Spine 2004; 29:2485-2492. 72. Harrison DE, Colloca CJ, Keller TS, Harrison DD, Janik TJ. Anterior thoracic posture increases thoracolumbar disc loading. Eur Spine J 2005:14:234-242. 73. McAviney J, Schulz D, Richard Bock R, Harrison DE, Holland B. Determining a clinical normal value for cervical lordosis. J Manipulative Physiol Ther 2005;28:187-193. 74. Keller TS, Colloca CJ, Harrison DE, Harrison DD, Janik TJ. Morphological and Biomechanical Modeling of the Thoracoc-lumbar Spine: Implications for the Ideal Spine. Spine Journal 2005; 5:297-305. 75. Harrison DE, Haas JW, Harrison DD, Janik TJ, Holland B. Do Sagittal Plane Anatomical Variations (Angulation) of the Cervical Facets and C2 Odontoid Affect the Geometrical Configuration of the Cervical Lordosis? Results from Digitizing Lateral Cervical Radiographs in 252 neck pain subjects. Clin Anat 2005; 18:104-111.
Practice Protocols
76. Troyanovich SJ, Harrison DE, Harrison DD. Review of the Scientific Literature Relevant to Structural Rehabilitation of the Spine and Posture: Rationale for Treatment Beyond the Resolution of Symptoms. J Manipulative Physiol Ther 1998;21(1):37-50. 77. Troyanovich SJ, Harrison DD, Harrison DE. Low back pain and the lumbar intervertebral disc: Clinical considerations for the doctor of chiropractic. J Manipulative Physiol Ther 1999; 22(2): 96-104. 78. Harrison DE, Harrison DD, Troyanovich SJ. A Normal Spinal Position, Its Time to Accept the Evidence. J Manipulative Physiol Ther 2000; 23: 623-644. 79. Oakley PA, Harrison DD, Harrison DE, Haas, JW. Evidence-Based Protocol for Structural Rehabilitation of the Spine and Posture: Review of Clinical Biomechanics of Posture (CBP®) Publications. J Canadian Chiro Assoc 2005; 49(4):270-296. 80. Maltby JK, Harrison DD, Harrison DE, Betz JB, Ferrantelli JR, Clum GW. Program of Care Derived from Pain Data Reported in RCTs on Low Back Pain. J Vertebral Subluxation Research [February 14, 2009, pp 1-16]. 81. Maltby JK, Harrison DD, Harrison DE, Betz JW, Ferrantelli JR, Clum GW. Frequency & Duration of chiropractic care for headaches, neck, and upper back pain. JVSR 2008; August 21:1-12.
Posture Reliability & Validity Studies
82. Harrison DE, Janik TJ, Cailliet R, Harrison DD, Normand MC, Perron DL, Oakley PA. Pelvic posture as rotations and translations in three dimensions from three two-dimensional digital images. J Chiropractic Education 2006;20(1):18-19. 83. Normand MC, Descarreaux M, Harrison DD, Harrison DE, Perron DL, Ferrantelli JR, Janik TJ. Three dimensional evaluation of posture in standing with the PosturePrint: an intra- and inter-examiner reliability study. Chiropractic & Osteopathy 2007; Sept. 24th 15:15. 84. Lafond D, Descarreaux M, Harrison DD, Normand MC, Harrison DE. Postural development in school children: a cross-sectional study. Chiropr Osteopat 2007; Jan 4; 15:1. 85. Janik TJ, Harrison DE, Cailliet R, Harrison DD, Normand MC, Perron DL. Validation of an algorithm to estimate 3-D rotations and translations of the head in upright posture from three 2-D images. J Manipulative Physiol Ther 2007;30(2):124-129. 86. Harrison DE, Janik TJ, Cailliet R, Harrison DD, Normand MC, Perron DL, Ferrantelli JR. Validation of an algorithm to estimate 3-D rotations and translations of the rib cage in upright posture from three 2-D digital images. Eur Spine J 2007; 16(2):213-218. 87. Harrison DE, Janik TJ, Cailliet R, Harrison DD, Normand MC, Perron DL, Oakley PA. Upright static pelvic posture as rotations and translations in 3-dimensional from three 2-dimensional digital images: validation of a computerized analysis. J Manipulative Physiol Ther 2008 Feb;31(2):137-45.
Reviews of the Literature
88. Harrison DD, Troyanovich SJ, Harrison DE, Janik TJ, Murphy DJ. A Normal Sagittal Spinal Configuration: A Desirable Clinical Outcome. J Manipulative Physiol Ther 1996;19(6):398-405. 89. Harrison DE, Harrison DD, Troyanovich SJ. The Sacroiliac Joint: A Review of Anatomy and Mechanics. J Manipulative Physiol Ther 1997; 20(9): 607-17. 90. Harrison DE, Harrison DD, Troyanovich SJ. Three-Dimensional Spinal Coupling Mechanics. Part I: A Review of the Literature. J Manipulative Physiol Ther 1998; 21(2): 101-113. 91. Harrison DE, Harrison DD, Troyanovich SJ. Three-Dimensional Spinal Coupling Mechanics. Part II: Implications for Chiropractic Theories and Practice. J Manipulative Physiol Ther 1998; 21(3): 177-86 . 92. Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART I: Spinal Canal Deformations Due to Changes in Posture. J Manipulative Physiol Ther 1999; 22(4):227-234. 93. Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART II: Strains in the Spinal Cord from Postural Loads. J Manipulative Physiol Ther 1999; 22(5):322-332. 94. Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART III: Spinal Cord Stresses from Postural Loads and Their Neurologic Effects. J Manipulative Physiol Ther 1999; 22(6):399-410. 95. Harrison DD, Harrison SO, Croft AC, Harrison DE, Troyanovich SJ. Sitting Biomechanics Part I: Review of the Literature. J Manipulative Physiol Ther 1999; 22(9): 594-609. 96. Harrison DD, Harrison SO, Croft AC, Harrison DE, Troyanovich SJ. Sitting Biomechanics Part II: Optimal Car Driver’s Seat and Optimal Driver’s Spinal Model. J Manipulative Physiol Ther 2000; 23(1): 37-47. 97. Oakley PA, Harrison DD, Harrison DE, Haas JW. On "phantom risks" associated with diagnostic ionizing radiation: evidence in support of revising radiography standards and regulations in chiropractic. J Canadian Chiro Assoc 2005; 49(4):264-269. 98. Harrison DE, Harrison DD, Oakley PA, Haas JW. Use of fallacious arguments, ad hominem attacks, and biased ‘expert opinions’ can make CBP research ‘appear flawed’. J Canadian Chiro Assoc 2006; 50(3): 99. Oakley PA, Harrison DD, Harrison DE, Haas JW. A rebuttal to Chiropractic Radiologists’ view of the 50-year-old linear-no-threshold radiation risk model. J Canadian Chiro Assoc 2006; 50(3):172-181. 100. Oakley PA, Betz JW, Haas JW. A history of spine traction. JVSR 2007;Mar 2:1-12. 101. Harrison DE, Betz J, Ferrantelli JF. Sagittal spinal curves and health. JVSR 2009 July 31, pp 1-8.
Critical Appraisal of Chiropractic Methods
102. Harrison DD, Colloca CJ, Troyanovich SJ, Harrison DE. Torque: An Appraisal of Misuse of Terminology in Chiropractic Literature and Technique. J Manipulative Physiol Ther 1996;19(7): 454-462. 103. Harrison DE, Harrison DD, Troyanovich SJ. Reliability of Spinal Displacement Analysis on Plane X-rays: A Review of Commonly Accepted Facts and Fallacies with Implications for Chiropractic Education and Technique. J Manipulative Physiol Ther 1998;21:252-66. 104. Troyanovich SJ, Harrison DD, Harrison DE. Commentary, Motion Palpation: It’s Time to accept the evidence. J Manipulative Physiol Ther 1998; 21(8): 569-571. 105. Harrison DD, Colloca CJ, Troyanovich SJ, Harrison DE. Commentary, Torque Misuse Revisited. J Manipulative Physiol Ther 1998; 21(9): 649-655.
X-Ray Projection
106. Coleman RR, Bernard BB, Harrison DE. The Effects of Real Life X-axis Vertebral Translation on Projected Y-axis Vertebral Rotation Images. J Manipulative Physiol Ther 1998;21:333-40. 107. Coleman RR, Bernard BB, Harrison DE, Harrison SO. Correlation and quantification of projected 2-D radiographic images with actual 3-D y-axis vertebral rotations. J Manipulative Physiol Ther 1999; 22(1): 21-25. 108. Coleman RR, Harrison DE, Fischer T, Harrison SO. Correlation and Quantification of Relative 2-D Projected Vertebral Endplate Z-axis Rotations with 3-D Y-axis Vertebral Rotations and Focal Spot Elevation. J Manipulative Physiol Ther 2000; 23(6): 414-419. 109. Coleman RR, Harrison DE, Bernard BB. The Effects of Combined X-axis Translations and Y-axis Rotations on Projected Lamina Junction Offset. J Manipulative Physiol Ther 2001; 24(8): 509-513.
Spinal Coupling / Kinematics Under Posture & Manipulative Thrusts
110. Harrison DE, Cailliet R, Harrison DD, Janik TJ, Troyanovich SJ, Coleman RR. Lumbar Coupling During Lateral Translations of the Thoracic Cage Relative to a Fixed Pelvis. Clin Biomech 1999; 14(10): 704-709. 111. Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ. Cervical Coupling During Lateral Head Translations Creates an “S”-Configuration. Clin Biomech 2000; 15: 436-440. 112. Harrison DE, Harrison DD, Janik TJ, Holland B, Siskin L. Slight Head Extension: Does it Reverse the Cervical Curve? Euro Spine J 2001; 10: 149-153. 113. Harrison DE, Cailliet R, Harrison DD, Janik TJ. How Do Anterior/Posterior Translations of the thoracic cage affect the Sagittal Lumbar Spine, Pelvic Tilt, and Thoracic Kyphosis? Euro Spine J 2002; 11(3): 287-293. 114. Keller TS, Colloca CJ, Beliveau JG. Force-deformation response of the lumbar spine: a sagittal plane model of posteroanterior manipulation and mobilization. Clin Biomech 2002:17(3):185-96. 115. Colloca CJ, Keller TS, Black P, Normand MC, Harrison DE, Harrison DD. Comparison of mechanical force of manually assisted chiropractic adjusting instruments. J Manipulative Physiol Ther 2005;28(6):414-422. 116. Harrison DE, Betz JW, Cailliet R, Harrison DD, Haas JW, Janik TJ. Production of Radiographic Pseudo-Scoliosis from Lateral Thoracic Translation Posture (Trunk List). Archives Physical Medicine & Rehabil 2006; Jan;87(1):117-22. 117. Colloca CJ, Keller TS, Harrison DE, Moore RJ, Gunzburg R, Harrison DD. Spinal manipulation force and duration affect vertebral movement and neuromuscular responses. Clinical Biomechanics 2006; Mar;21(3):254-62. 118. Keller TS, Colloca CJ, Moore RJ, Gunzburg R, Harrison DE, Harrison DD. Three- dimensional intersegmental motion validation of mechanical force spinal manipulation. J Chiropractic Education 2006;20(1):27. 119. Colloca CJ, Keller TS, Harrison DE, Moore RJ, Gunzburg R, Harrison DD. Neuromuscular contributions to dynamic posteroanterior spinal stiffness. J Chiropractic Education 2006;20(1):6-7. 120. Keller TS, Colloca CJ, Moore RJ, Gunzburg R, Harrison DE, Harrison DD. Three- dimensional vertebral motions produced by mechanical force spinal manipulation. J Manipulative Physiol Ther 2006 Jul-Aug;29(6):425-36. 121. Keller TS, Colloca CJ, Moore RJ, Gunzburg R, Harrison DE. Increased multiaxial lumbar motion responses during multiple-impulse mechanical force manually assisted spinal manipulation. Chiropratic & Osteopathy 2006; 14(1):6-14. 122. Keller TS, Colloca CJ, Harrison DE, Moore RJ, Gunzburg R. Muscular contributions to dynamic dorsoventral lumbar spine stiffness. European Spine Journal 2007; 16(2):245-54. 123. Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE. Intervertebral disc degeneration reduces vertebral motion responses. Spine 2007; 32(19):E544-50. 124. Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE. Effects of disc degeneration on neurophysiological responses during dorsoventral mechanical excitation of the ovine lumbar spine. Journal of Electromyography and Kinesiology 2008;18(5):829-37. 125. Gunzburg R, Szpalski M, Callary SA, Colloca CJ, Kosmopoulos V, Harrison DE, Moore RJ. Effect of a novel interspinous implant on lumbar spinal range of motion. Eur Spine J 2009;18:696-703.
1 Harrison DD. CBP Technique: The Physics of Spinal Correction. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction.
2 Harrison DD. Spinal Biomechanics: A Chiropractic Perspective. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction.
3 Harrison DD. CBP X-ray Work Book. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction.
4 Harrison DE, Harrison, DD, Haas JW. CBP® Structural Rehabilitation of the Cervical Spine. Evanston, WY: Harrison CBP Seminars, 2002.
5 Harrison DE, Harrison, DD, Haas JW, Oakley PA. Spinal Biomechanics for Clinicians, Volume I. Evanston, WY: Harrison CBP Seminars, 2003.
6 Harrison DE, Harrison, DD, Haas JW, Oakley PA. CBP® Structural Rehabilitation of the Lumbar Spine. Evanston, WY: Harrison CBP Seminars, 2005.
7 Harrison DE, Betz J, Harrison, DD. CBP® Structural Rehabilitation of the Thoracic Spine. Evanston, WY: Harrison CBP Seminars, 2005.
8 Chiropractic Biophysics Online. https://idealspine.com/. Services/research papers. Accessed 12-15-04.
9 Harrison DD, Janik TJ, Harrison GR, Troyanovich SJ, Harrison DE, Harrison SO. Chiropractic Biophysics Technique: A Linear Algebra Approach to Posture in Chiropractic. J Manipulative Physiol Ther 1996;19(8):525-535.
10 Panjabi MM, White AA, Brand RA. A Note on Defining Body Parts Configurations. J Biomech 1974; 7:385.
11 Harrison DE, Harrson DD. The Lumbar Spine: Rehabilitation with the CBPâ method. National Library of Medicine #WE 725 4318C, 1997.
12 Harrison DE, et al. Changes in sagittal lumbar configuration with a new method of extension traction. Presented at the 27th annual meeting of the International Society for the Study of the Lumbar spine. Adelaide, Australia April 9-13, 2000;151.
13 Harrison DE, Harrison DD, Cailliet R, Janik TJ, Holland B. Changes in Sagittal Lumbar Configuration with a New Method of Extension Traction: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002;83(11):1585-1591.
14 Harrison DD, Jackson BL, Troyanovich SJ, Robertson GA, DeGeorge D, Barker WF. The Efficacy of Cervical Extension-Compression Traction Combined with Diversified Manipulation and Drop Table Adjustments in the Rehabilitation of Cervical Lordosis. J Manipulative Physiol Ther 1994;17(7):454-464.
15 Harrison DE, Harrison DD, Betz J, Colloca CJ, Janik TJ, Holland B. Increasing the Cervical Lordosis with Seated Combined Extension-Compression and Transverse Load Cervical Traction with Cervical Manipulation: Non-randomized Clinical Control Trial. J Manipulative Physiol Ther 2003; 26(3): 139-151.
16 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. New 3-Point Bending Traction Method of Restoring Cervical Lordosis Combined with Cervical Manipulation: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002; 83(4): 447-453.
17 Harrison DE, Cailliet R, Betz JW, Harrison DD, Haas JW, Janik TJ, Holland B. Harrison Mirror Image Methods for Correcting Trunk List: A Non-randomized Clinical Control Trial. Eur Spine J 2004; In Press.
18 Harrison DE, Harrison DD, Haas JW, Betz JW, Janik TJ, Holland B. Conservative Methods to Correct Lateral Translations of the Head: A Non-randomized Clinical Control Trial. J Rehab Res Devel 2004;41(4):631-640.
19 Zaleski BW, Wood J. A comparison of Palmer package and Chiropractic Biophysics for the treatment of pain. Proceedings of the International Conference on Spinal Manipulation 1992; Chicago, IL., May 15-17.
20 Paulk GP, Bennett DL, Harrison DE. Management of a chronic lumbar disk herniation with CBP methods following failed chiropractic manipulative intervention. J Manipulative Physiol Ther 2005;in press.
21 Ferrantelli JR, Harrison DE, Harrison DD, Steward D. Conservative management of previously unresponsive whiplash associated disorders with CBP methods: a case report. J Manipulative Physiol Ther 2005;in press.
22 Haas JW, Harrison DE, Harrison DD, Bymers B. Reduction of symptoms in a patient with syringomyelia, cluster headaches, and cervical kyphosis. J Manipulative Physiol Ther 2005;in press.
23 Harrison DE, Bula J. Non-operative correction of the flexible flat back using lumbar extension traction: A case study of three. J Chiropractic Education 2002;16(1).
24 Bastecki A, Harrison DE, Haas JW. ADHD: A CBP case study. J Manipulative Physiol Ther 2004; 27(8):e14.
25 Harrison DE, Harrison DD. Chiropractic Biophysics Technique. Part I: The Scientific Basis. Eur Chiropractic J 2005;
26 Harrison DD, Janik TJ, Troyanovich SJ, Holland B. Comparisons of Lordotic Cervical Spine Curvatures to a Theoretical Ideal Model of the Static Sagittal Cervical Spine. Spine 1996;21(6):667-675.
27 Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW, Ferrantelli J, Holland B. Modeling of the Sagittal Cervical Spine as a Method to Discriminate Hypo-Lordosis: Results of Elliptical and Circular Modeling in 72 Asymptomatic Subjects, 52 Acute Neck Pain Subjects, and 70 Chronic Neck Pain Subjects. Spine 2004; 29:2485-2492.
28 Janik TJ, Harrison DD, Cailliet R, Troyanovich SJ, Harrison DE. Can the Sagittal Lumbar Curvature be Closely Approximated by an Ellipse? J Orthop Res 1998; 16(6):766-70.
29 Harrison DD, Cailliet R, Janik TJ, Troyanovich SJ, Harrison DE, Holland B. Elliptical Modeling of the Sagittal Lumbar Lordosis and Segmental Rotation Angles as a Method to Discriminate Between Normal and Low Back Pain Subjects. J Spinal Disord 1998; 11(5): 430-439.
30 Harrison DE, Janik TJ, Harrison DD, Cailliet R, Harmon S. Can the Thoracic Kyphosis be Modeled with a Simple Geometric Shape? The Results of Circular and Elliptical Modeling in 80 Asymptomatic Subjects. J Spinal Disord Tech 2002; 15(3): 213-220.
31 Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW. Do Alterations in Vertebral and Disc Dimensions Affect an Elliptical Model of the Thoracic Kyphosis? Spine 2003; 28(5):463-469.
32 Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ. Cobb Method or Harrison Posterior Tangent Method: Which is Better for Lateral Cervical Analysis? Spine 2000; 25: 2072-78.
33 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Centroid, Cobb or Harrison Posterior Tangents: Which to Choose for Analysis of Thoracic Kyphosis? Spine 2001; 26(11): E227-E234.
34 Harrison DE, Harrison DD, Janik TJ, Harrison SO, Holland B. Determination of Lumbar Lordosis: Cobb Method, Centroidal Method, TRALL or Harrison Posterior Tangents? Spine 2001; 26(11): E236-E242.
35 Harrison DE, Holland B, Harrison DD, Janik TJ. Further Reliability Analysis of the Harrison Radiographic Line Drawing Methods: Crossed ICCs for Lateral Posterior Tangents and AP Modified Risser-Ferguson. J Manipulative Physiol Ther 2002; 25: 93-98.
36 Harrison DE, Harrison DD, Colloca CJ, Betz J, Janik TJ, Holland B. Repeatability of Posture Overtime, X-ray Positioning, and X-ray Line Drawing: An Analysis of Six Control Groups. J Manipulative Physiol Ther 2003; 26(2): 87-98.
37 Haas M, Taylor JAM, Gillette RG. The routine use of radiographic spinal displacement analysis: a dissent. J Manipulative Physiol Ther 1999;22:254-259.
38 Phillips RB. Plain film radiography in chiropractic. J Manipulative Physiol Ther 1992;15:47-50.
39 Taylor JAM. Full-spine radiography: a review. J Manipulative Physiol Ther 1993;16:460-474.
40 Kauffman JM. Diagnostic radiation: are the risks exaggerated? J Amer Phys Surg 2003;8(2):54-55.
41 Cohen BL, Lee IS. A catalog of risks. Health Physics 1979;36:707-722.
42 International Atomic Energy Agency. Facts about low-level radiation. American Nuclear Society, 1982.
43 Janik TJ, Harrison DE, Cailliet R, Harrison DD, Normand MC, Black P. Validity of an algorithm to estimate 3-D rotations and translations of the head in upright posture from three 2-D digital images. 2005; In Review.
44 Harrison DE, Janik TJ, Cailliet R, Harrison DD, Normand MC, Black P, Perron DL. Validation of an algorithm to estimate 3-D rotations and translations of the thorax and pelvis in upright posture from three 2-D digital images. 2005 In Review.
45 Bolton JE. The evidence in evidence-based practice: what counts and what doesn’t count? J Manipulative Physiol Ther 2001;24:362-366.
46 Hrysomallis C, Goodman C. A review of resistance exercise and posture realignment. J Strength Cond Res 2001;15:385-390
47 Den Boer WA, Anderson PG, Limbek JV, Kooijman MAP. Treatment of idiopathic scoliosis with side shift therapy: An initial comparison with a brace treatment historical cohort. European Spine J 1999;8:406-410.
48 Weiss HR. Influence of an in-patient exercise program on scoliotic curve. Ital J Orthop Traumatol 1992; 18:395-406.
49 Weiss HR, Lohschmidt K, el-Obeidi N, Verres C. Preliminary results and worst-case analysis of in patient scoliosis rehabilitation. Pediatr Rehabil 1997;1:35-40.
50 Pearson ND, Walmsley RP. Trial into the effects of repeated neck retractions in normal subjects. Spine 1995; 20(11): 1245-51.).
51 DeVocht JW, Pickar JG, Wilder DG. EMG activity levels of paraspinal muscles during spinal manipulation. Proceedings from the 29th annual meeting of ISSLS 2002; Vancouver, Canada.
52 Oliver MJ, Twomey LT. Extension creep in the lumbar spine. Clin Biomech 1995;10:363-368.
53 Harrison DE, Harrison DD, Troyanovich SJ. Three-Dimensional Spinal Coupling Mechanics. Part II: Implications for Chiropractic Theories and Practice. J Manipulative Physiol Ther 1998; 21(3): 177-86.
54 Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Janik TJ. Cervical Coupling on AP Radiographs During Lateral Translations of the Head Creates an S-Configuration. Clin Biomech 2000; 15(6): 436-440.
55 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Troyanovich SJ, Coleman RR. Lumbar Coupling During Lateral Traction.
